



Memory Loss Isn't the First Warning
The popular image of Alzheimer's disease begins with forgetting names, appointments, conversations. That framing is understandable — memory loss is the symptom that disrupts daily life enough to bring someone to a clinic.
But the biological process starts earlier. Considerably earlier. And it doesn't begin in the memory system.
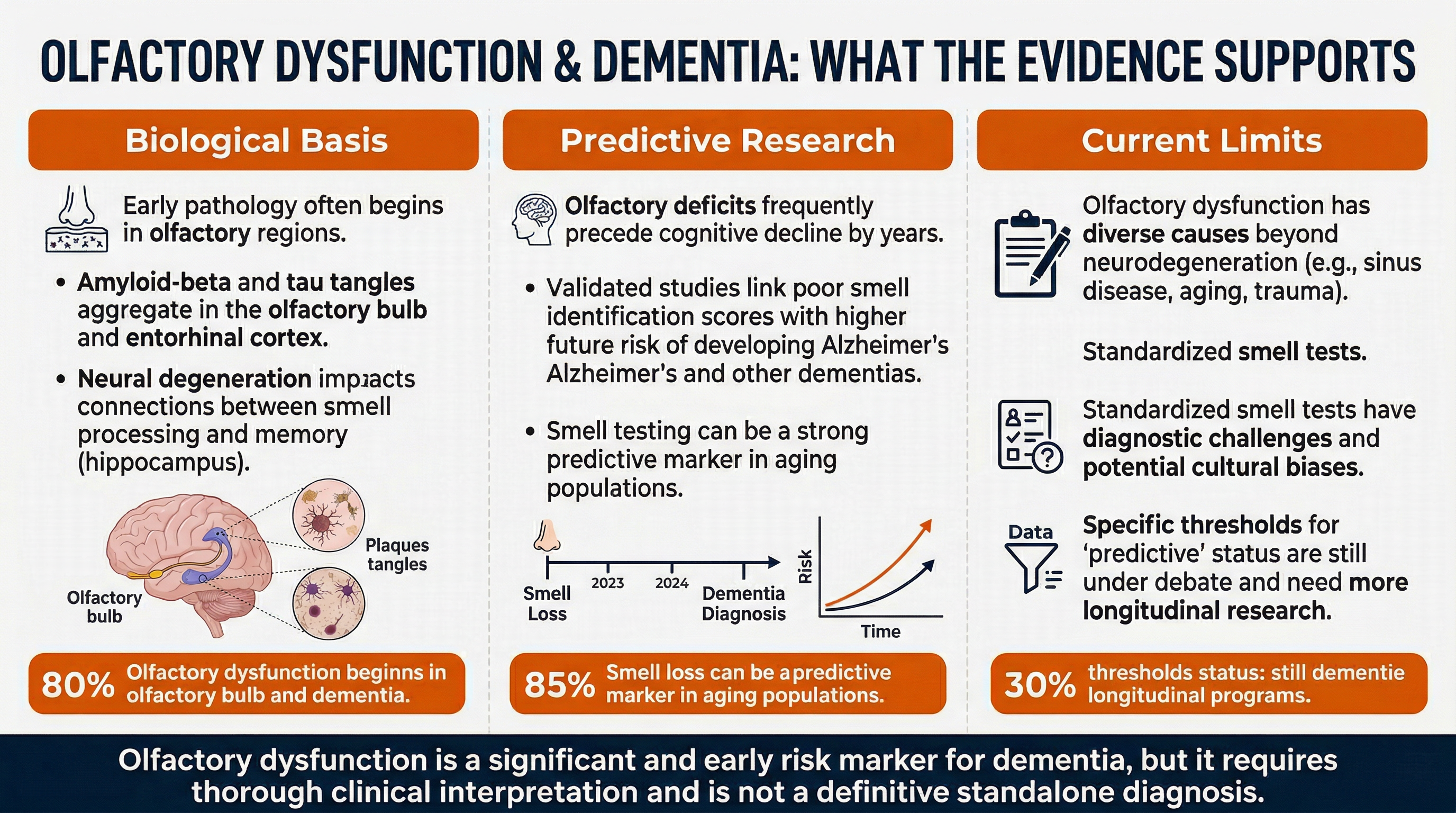
Evidence from post-mortem and neuroimaging studies shows that amyloid-beta plaques and tau tangles — the molecular signatures of Alzheimer's disease — accumulate in olfactory brain structures before they reach hippocampal and cortical memory regions. The anterior olfactory nucleus and piriform cortex, both critical to smell processing, show pathological changes in the preclinical stage of the disease. Memory-related brain regions are targeted later.
This sequence gives researchers a theoretical detection window — a period when biological damage is occurring but no cognitive symptoms have emerged. Smell-based screening has attracted serious scientific attention for exactly this reason.
---
What the Research on Smell Tests Actually Shows
Objective, standardized smell identification tests — validated odor identification batteries administered under normed clinical conditions — have demonstrated the ability to predict dementia risk in large prospective cohort studies. Some of these studies tracked participants for 6 to 12 years before cognitive decline appeared, observing that lower baseline olfactory scores correlated with higher later risk.
This is a meaningful finding. It suggests the biological relationship between olfactory decline and neurodegeneration is not coincidental.
One critical distinction matters here, however: self-reported smell loss is not the same as objectively measured olfactory dysfunction. Asking someone "has your sense of smell gotten worse?" carries insufficient validity for any clinical risk assessment. The studies that show predictive power use standardized protocols — not questionnaires.
---
What Olfactory Dysfunction Is — and Is Not
Olfactory dysfunction is a probabilistic risk biomarker for dementia. That phrase is precise and important.
A risk biomarker means it is associated with elevated statistical risk. It does not confirm disease. It does not predict with certainty. It is not diagnostic.
No regulatory body — including the FDA — has approved any olfactory test as a standalone instrument to diagnose dementia or Alzheimer's disease. The clinical application of smell-based screening remains an active research area. Promising biology does not equal approved diagnostic tool.
This distinction is frequently blurred in media coverage, generating unnecessary alarm in people who notice any change in their sense of smell.
---
The More Common Explanation for Smell Loss
The vast majority of olfactory dysfunction has nothing to do with neurodegeneration. Smell loss is a common symptom with a long list of reversible and benign causes:
- Upper respiratory infections — the most frequent short-term cause
- Chronic allergies and rhinitis — ongoing nasal inflammation reduces odor detection
- Nasal polyps — non-cancerous growths that physically block olfactory access
- Medications — a wide range of commonly prescribed drugs affect smell as a side effect
- COVID-19 sequelae — post-viral olfactory loss has affected a large population since 2020
- Nutritional deficiencies — zinc deficiency in particular is associated with impaired olfaction
- Normal aging — olfactory sensitivity declines gradually with age, independent of neurodegeneration
All of these causes must be systematically excluded before attributing smell loss to any neurodegeneration risk. The COVID-19 pandemic in particular has created a large population with acquired olfactory dysfunction that carries no inherent dementia signal.
---
A Future Direction Worth Watching
Researchers are investigating whether olfactory neurons — sampled via a nasal brushing — may carry detectable tau and amyloid-beta proteins. If validated, this approach could provide a minimally invasive screening method that avoids lumbar puncture or expensive neuroimaging.
This science is in early stages. It has not been validated in large prospective trials and is not currently available as a clinical test. It represents a direction, not a destination.
---
What to Do with This Information
If you or a family member have noticed persistent, unexplained smell loss — not connected to a recent infection, allergy season, or medication change — that is a data point worth discussing with a physician.
Not as evidence of dementia. Not as a reason for alarm. As a flag that belongs in a clinical conversation, where reversible causes can be assessed systematically and, if needed, appropriate further investigation considered.
The science of early detection is evolving. Early conversations with a doctor remain the most actionable step available today.
---
Disclaimer: This content is for educational purposes only and does not constitute medical advice. We do not diagnose or treat any condition. Always consult a qualified healthcare provider for personalized recommendations about supplements, dosage, and potential interactions.
Sources
- Somatostatin, tau, and beta-amyloid within the anterior olfactory nucleus in Alzheimer disease - PubMed
- Olfaction deterioration in cognitive disorders in the elderly - PubMed
- Alzheimer Disease - PubMed
- FDA Drug Evaluation and Research - Alzheimer's Disease Application Review 2024
- FDA Center for Drug Evaluation and Research - Biomarker Framework Document
- Olfactory Deficits and Treatment in Cognitively Impaired Patients - ClinicalTrials Protocol
- Smell, Voice and Nasal Swabs as Markers for Neurodegeneration - ClinicalTrials Protocol
- Smell Retraining Study - Sniffin Sticks Protocol Reference
- FDA Guidance: Chronic Rhinosinusitis With Nasal Polyps - Drug Development