



Potassium Deficiency and Hypertension: The Two Mechanisms Your Doctor May Not Have Mentioned
Blood pressure advice has been dominated by a single instruction for decades: eat less salt. That advice is evidence-based and correct. It is also incomplete.
The missing half of the conversation is potassium — a mineral classified by health authorities as a nutrient of public health concern, chronically under-consumed by most adults in the developed world, and mechanistically linked to blood pressure through two entirely independent pathways.
---
The Potassium Shortfall Is Larger Than Most People Realize
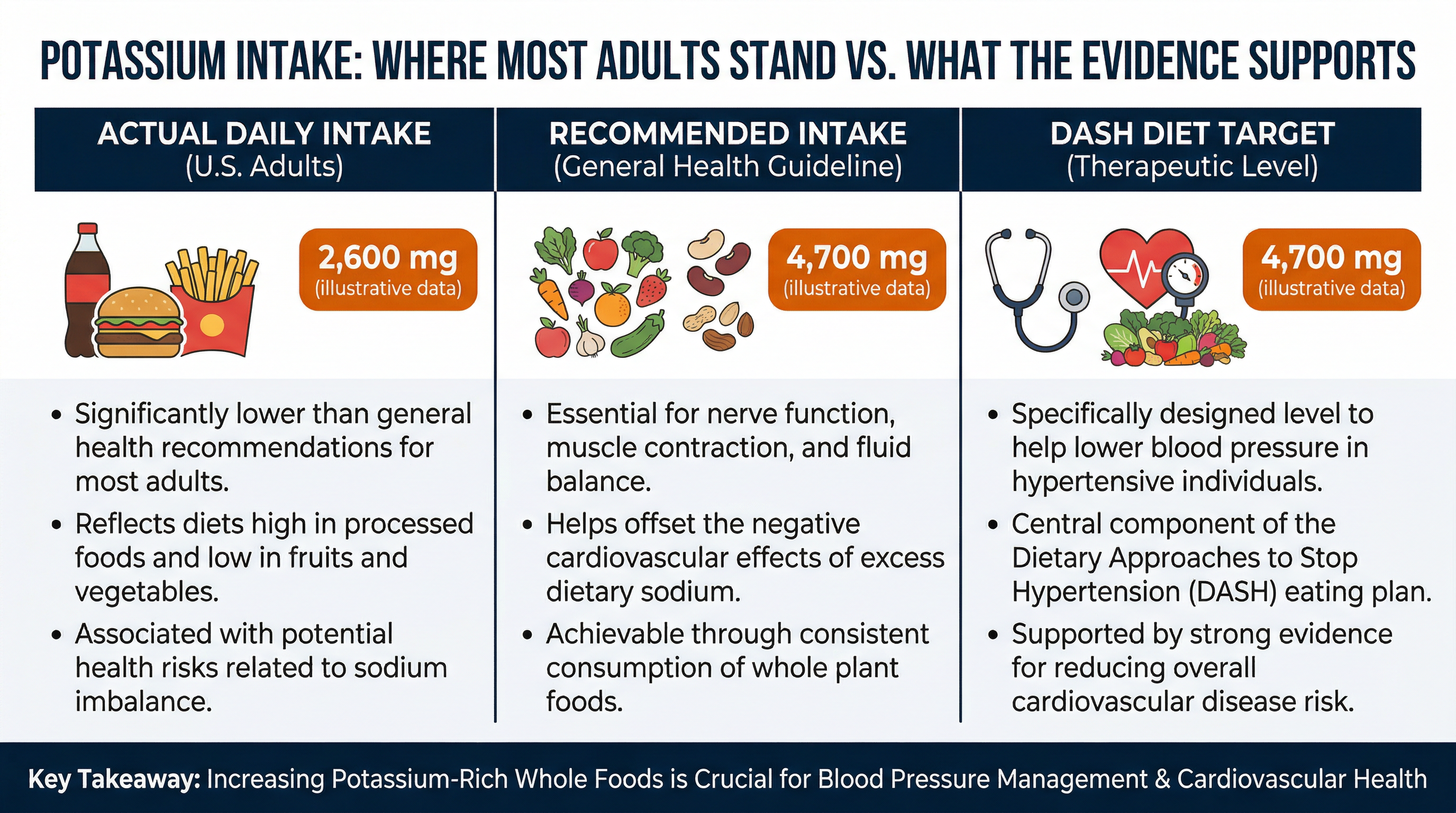
The recommended adequate intake of potassium is 2,600 mg per day for women and 3,400 mg per day for men. The median American adult consumes less than 2,500 mg — falling short of the minimum recommendation for both sexes.
The DASH (Dietary Approaches to Stop Hypertension) dietary pattern, which has demonstrated clinically meaningful blood pressure reductions in randomized controlled trials, targets 4,700 mg per day from whole foods. That is nearly double what most people currently eat.
This shortfall is not a rounding error. It represents a significant, population-level gap between what the cardiovascular system operates optimally on and what most people actually deliver to it.
---
How Potassium Controls Blood Pressure: Mechanism One — The Kidney
Potassium promotes natriuresis — the excretion of sodium through the kidneys. When potassium intake is adequate, the kidneys receive the signaling support they need to flush excess sodium from the body. When potassium is low, this process weakens. Sodium accumulates in the bloodstream, blood volume expands, and pressure rises.
This is why cutting sodium and increasing potassium work better together than either strategy does alone. They address the same problem from opposite ends of the same equation. The natriuretic effect of potassium varies by individual sodium sensitivity and baseline intake, but the directional evidence is consistent across multiple study designs.
---
How Potassium Controls Blood Pressure: Mechanism Two — The Vessel Wall
Separate from kidney function, potassium directly influences the tension in blood vessel walls. It does this by hyperpolarizing vascular smooth muscle cells — essentially changing their electrical state so that calcium channels close. Calcium entry into smooth muscle is what drives contraction and arterial stiffness. Block it, and the vessel relaxes.
This vasodilatory mechanism operates independently of the kidney pathway. It means potassium's cardiovascular benefit cannot be fully replicated by sodium restriction alone, because the two mechanisms target different physiological processes.
---
The Self-Reinforcing Cycle: Potassium Deficiency and RAAS Activation
Chronically low potassium intake can activate the renin-angiotensin-aldosterone system (RAAS) — the body's hormonal pressure-raising cascade. Aldosterone, one of the hormones in this system, drives sodium retention and simultaneously promotes further potassium loss through the kidneys.
The result is a self-reinforcing cycle: low potassium triggers RAAS, RAAS depletes potassium further, blood pressure rises, and the deficit deepens. Most of the direct evidence for this mechanism comes from clinical hypertension populations rather than healthy adults, but the pathway is mechanistically established and practically relevant: early correction of low potassium intake matters more than waiting for symptoms to appear.
---
The Ratio That Predicts Risk Better Than Sodium Alone
Research — including WHO meta-analyses and multiple observational cohort studies — has identified the sodium-to-potassium ratio in the diet as a stronger independent predictor of cardiovascular risk and blood pressure than either sodium or potassium measured in isolation.
This finding reframes the practical strategy. The goal is not simply to eat less of one thing. It is to restore balance between two minerals that most modern diets have dramatically skewed toward sodium. When reading nutrition labels, checking the sodium content is useful — but checking the sodium-to-potassium balance of a food gives a more complete cardiovascular picture.
---
Why Supplements Cannot Solve This
Over-the-counter potassium supplements are subject to regulatory dose limits per tablet. These limits exist for legitimate safety reasons: high-dose oral potassium can cause gastrointestinal injury, and excessive blood potassium (hyperkalemia) carries serious cardiac risks. The result is that standard store-bought supplements deliver doses too small to meaningfully close a dietary gap of 2,000+ mg per day.
Prescription-strength potassium formulations exist and are used clinically — particularly for patients on diuretics who lose potassium through medication — but these require medical supervision.
For most people without a medical condition that alters potassium metabolism, the evidence-backed path is food-first.
---
The DASH Approach: What 4,700 mg Looks Like in Practice
The DASH dietary pattern reaches 4,700 mg of potassium per day through whole foods, not supplements. High-potassium foods include:
- Lentils and beans — one cup of cooked lentils delivers approximately 730 mg
- Potatoes — a medium baked potato with skin contains around 900 mg
- Leafy greens — Swiss chard, spinach, and beet greens are among the highest-density options
- Avocado — one cup provides approximately 700 mg
- Bananas — useful, though more moderate at around 420 mg per fruit
The DASH pattern also reduces sodium and saturated fat, which is why isolating potassium's specific contribution to its blood pressure benefit is methodologically difficult. What the evidence does support clearly is the overall pattern — and the whole-food potassium strategy that underpins it.
---
What to Do Today
The most practical step is also the most direct: add one high-potassium food to every main meal. That single habit — sustained — begins to shift the sodium-to-potassium ratio in the right direction without requiring radical dietary overhaul.
Pair that with continued attention to sodium reduction. The research is consistent: both strategies together produce greater blood pressure benefit than either alone.
The goal is not to hit 4,700 mg on day one. It is to start moving the ratio — and to understand that the conversation about blood pressure has always been about more than just salt.
---
- Modulation of blood pressure by dietary potassium and sodium
- Potassium restriction, blood pressure, and renal sodium retention (RCT)
- Age-period-cohort analysis: dietary sodium, potassium, and Na:K ratio
- Health effects of sodium and potassium in humans — meta-analysis
- WHO Potassium Intake Guidelines for Adults and Children
- Potassium channels in vascular smooth muscle
- Calcium regulation and vascular tone in hypertension
- DASH Diet RCT (NCT00000544)
--- Disclaimer: This content is for educational purposes only and does not constitute medical advice. We do not diagnose or treat any condition. Always consult a qualified healthcare provider for personalized recommendations about supplements, dosage, and potential interactions.
Sources
- Modulation of blood pressure by dietary potassium and sodium: sex differences and modeling analysis
- On the mechanism of the effects of potassium restriction on blood pressure and renal sodium retention
- Age-period-cohort analysis of dietary sodium, potassium, and sodium-to-potassium ratio in Korea
- Potassium intake for adults and children — WHO Guidelines
- Health effects of sodium and potassium in humans
- Sequential Nephron Blockade vs. Dual Blockade Renin-angiotensin System in Resistant Arterial Hypertension
- Potassium channels in vascular smooth muscle
- The role of calcium in the regulation of normal vascular tone and in hypertension
- The Use of an Alternate Name for Potassium Chloride in Food — FDA Guidance
- Using Digital Health to Improve Adherence to the DASH Diet — Trial Protocol
- Dietary Approaches to Stop Hypertension (DASH) — Original Trial
- Potassium Chloride Prescribing Information — FDA Label